Rubeotic Glaucoma (Neovascular Glaucoma) David Kinshuck |
This type of glaucoma follows a severe retinal vein blockage or severe diabetic eye disease. The animation here explains the condition if you are online, but this text is helpful if you need to print out a leaflet. |
|
|
Anatomy |
|
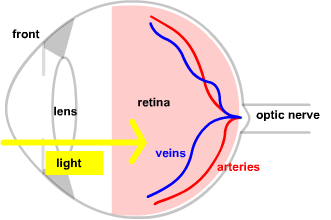
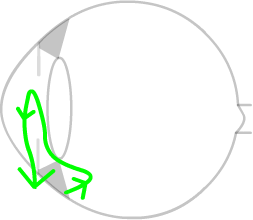
The healthy eye sees as light enters the eye and hits the retina. The 'retina' is the 'film' of the eye, just like the film of a camera. Blood travels through the optic nerve in arteries to reach the retina,
and is normally drained away out of the eye in veins.
|
|
|
The front chamber of the eye is filled with a clear watery fluid, the aqueous or (aqueous humour). The aqueous is made in the middle chamber of the eye, and flows through to the front chamber. It then flows through a drainage system, the 'trabecular meshwork', out of the eye into the blood stream. (It has nothing to do with tears.) |
 |
|
A retinal vein occlusion (blockage) |
|
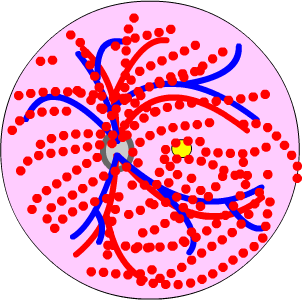
High blood pressure, smoking, glaucoma or an unhealthy diet may
damage the retinal veins. There is no treatment that will restore your sight after a retinal vein occlusion. Treatment, such as lowering blood pressure, is aimed at protecting the other eye or preventing other problems such as a stroke. About ½ the patients who develop a severe retinal vein occlusion will develop this rubeotic glaucoma condition. This diagram shows the retinal haemorrhages, in a photo here. If there is a lot of damage to your eye from diabetes you may also
get this condition....the process is very similar. It may also follow
other conditions, such as a 'total' retinal detachment. |
|
|
Rubeotic glaucoma (RG) |
|
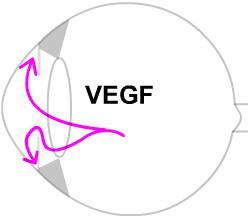
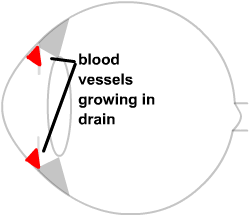
This damaged or 'sick' retina produces growth chemicals, call growth
factors. The growth chemicals spread to the front of the eye. Here they reach
the drainage system (the trabecular meshwork). |
|
|
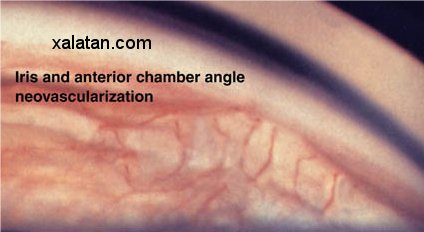
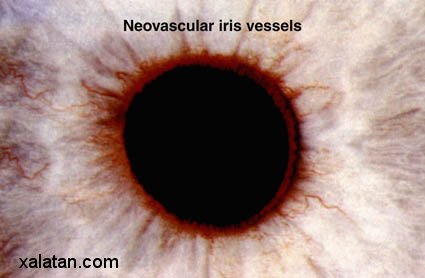
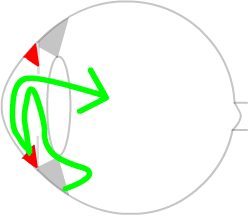
Here the VEGF makes tiny blood vessels grow, which we call 'new blood vessels'. At about the same time the blood vessels grow in the drainage system, they grow on the surface of the iris, where your doctor can see them. |
 |
|
These tiny blood vessels then block the drainage meshwork, so the aqueous fluid cannot leave the eye. As the fluid cannot escape, the pressure goes up, like a tyre being pumped up too much. The eye cannot burst, but it becomes much harder. In a way this is a 'faulty healing process'. |
 |
|
Treatment: laser& drops |
|
Without laser treatment this condition can lead to a painful blind
eye in about ½ the people affected. Luckier people have the
condition but there is no pain. With laser treatment, when the 'sick' ischaemic retina is lasered,
it stops producing the VEGF growth chemical. Without the VEGF, the
tiny blood vessels growing in the trabecular meshwork stop growing. Several thousand retinal laser burns are needed, in 3-5 sessions. If the drainage angle is scarred, Cyclodiode laser may be needed. Drops may help in this condition at the beginning. These include steroid eye drops such as Dexamethasone, and drops to dilate the pupil, such as atropine. Generally, these are only used for a few months, as they have many side effects if used for longer. Atropine makes your mouth dry and must be kept away from children. See animation. A new treatment, injection of anti-growth factors, is likely to be very helpful. Avastin is cheap and very helpful, although a series of injections may be needed. The drug is injected in to the vitreous cavity of the eye (identical to this treatment for ARMD) . Avastin is not yet licensed for this use...it has proved very helpful, but it is too early to say for certain. It is standard treatment in the US and is available in many private clinics in the UK. If you want Avastin you will have to ask your ophthalmologist. There are other drugs, Macugen and Lucentis, which are likely to be very effective also, but these are more expensive (£~600/injection), and there is very little published for these drugs in RG. See papers. Traditionally RG has been a very serious condition and they eye often does not recover its sight, but with these new treatments sight is more liely to improve. The injection will be needed early, as soon as possible after the condition is daigosed. Almost certainly laser will still be needed AS WELL. If you want Avastin in the UK on the NHS your ophthalmologist will have to get funding from your Primary Care Trust (PCT). About half of PCTs will fund Avastin for this use, half will not. The drug is not particularly expensive, but the injection procedure in a clean room has risks and costs the NHS £3-700. As Avastin is not licenced, it is not being studied by NICE, and unless this changes will never be made widely available on the NHS. There is no prospect of it being widely available for RG without this changing..we urgently need scientific studies to confirm that it works (or does not work), but there is no funding for the studies. If the studies showed that it was effective it would obtain a licence, and then NICE would consider it. |
|
Controversies in this condition |
| Many doctors prefer to laser early in this condition. That is they
laser all patients with a very severe retinal vein occlusion. But of
course not all these patients would develop rubeotic glaucoma. So that
means 100 patients will have to be lasered to prevent 50 from getting
rubeotic glaucoma. Even with laser a few patients, perhaps 5, will
still develop rubeotic glaucoma, but laser will prevent 45.
Other doctors, and the Royal College of Ophthalmologists, recommend
waiting till rubeotic glaucoma (or at least the blood vessel growth
on the iris and trabecular meshwork) develops, and then carry out
the laser. But unfortunately treatment at this stage is not always
successful. The author of this page prefers early laser, but knows
many experts who prefer waiting for the rubeosis. If you see 6/24 (20/80) or better you have a small risk and may often be fine without laser. If you see 6/36 (20/120) there is an intermediate risk. For professionals see and here with photos. Basic explanation here, medline, search. |
|
|
| The address of this site ('org' changing to 'nhs') is changing from http://www.goodhope.org.uk/departments/eyedept/ to http://www.goodhope.nhs.uk/departments/eyedept/ |
|