Intraocular hypertension David Kinshuck |
|
What is ‘intraocular hypertension’? |
|
How does this affect your sight? |
|
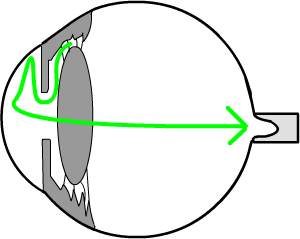
Generally your sight will be normal in this condition. But the condition is important, as sometimes you may develop ‘glaucoma’. A few people with intraocular hypertension develop glaucoma each year; this occurs when the pressure on the nerve at the back of the eye actually damages the nerve. In ‘intraocular hypertension’ the nerve at the back of the eye remains healthy. But in glaucoma the fluid pressure in the eye starts to press to hard on the nerve and damages it: this damages your sight. (The nerve is the ‘electric wire’ of the eye. It takes the messages from the eye about what you see, and sends them on to the brain.) |
If the drain blocks, the pressure in the eye builds up and may press on the nerve at the back of the eye, damaging the nerve and the sight. enlarge |
What do you need to do? |
| Your ophthalmologist
or optometrist need to check your eyes regularly, in order to check that glaucoma
has not developed. Generally you need yearly checks.
You need the three tests:
Eye Pressure As opposite, the tonometer probe touches the surfcae of the eye to measure the pressure. This takes a few seconds. |
measuring eye pressure is painless. After some anaesthetic drops, the 'tonometer' touches the surface of the eye. |
Ophthalmoscopy of the optic nerve The doctor looks at the optic nerve with an ophthalmoscope, a type of torch. This takes a few seconds. Often this test is carrried out whilst you are sitting at a slit lamp'. The slip lamp is simply a pair of binoculars with a light that shines in from the side. Visual field test A visual field test takes a little longer. It is a test to see that the nerve at the back of your eye is working properly. You have to sit with your head still looking straight ahead, and a light flashes from the side. If you see all the lights of a certain brightness, you press a button, and the computer keeps a record. it then prints out a 'map' of all the lights you can and cannot see, This test identifies whether or not the nerve is damaged. |
Who needs treatment |
You will not know whether you
have glaucoma in its early stages: this can only be detected by this
examination. Glaucoma does not cause pain. In practice many patients
are recommended treatment. Those with the lowest pressure (eg 22mmHg, and none of these risk factors), may not need treatment. Many patients are 'in between' and a personal discussion may be helpful. See more evidence and a search. The increased risk for Afrocarribean's is more related to the increase risk factors, rather than 'race' itself (Delaying...2010). Older patients with slightly high pressures (<24) without risk factors do not need treatment (Delaying...2010). There are of course many patients in between. |
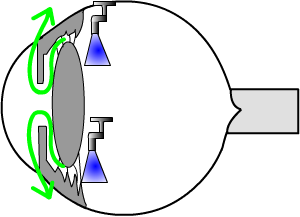
What is the cause of intraocular hypertension? |
| No one knows exactly why
the drain of the eye blocks. (It is the blocked drain keeping the
fluid inside the eye that causes the pressure in the eye to go up.)
See animation.
The blockage is not caused by smoking or anything you have done. However, the condition can run in the family. Scientists have found genes that can cause the condition. The genes, which you inherit from your parents, control the chemistry of the tiny cells in the ‘drain’. The cells may work normally for 50 years, letting the fluid out of the eye, but then begin to stop working. The fluid then gets trapped in the eye. Patients with intraocular hypertension who develop a retinal vein occlusion need to be treated as though they have early glaucoma, and need a low pressure. |
Your general health in glaucoma/intraocular hypertension |
|
Remember that your general health and lifestyle have a major impact on glaucoma and your sight. BJO 12
|
Summary |
| Intraocular hypertension
is a condition when the eye has a little too much fluid inside it,
like a tyre being pumped up too hard. It is not harmful itself, but
a few patients later develop glaucoma. Glaucoma
is more serious, as the fluid pressure in the eye presses on the nerve
at the back. This can damage your sight.
To detect glaucoma in the very early stages, you need three tests at your optometrists each year:
You should look after your general health, and your brothers and sisters should be also be tested by their optometrist. |
| Small print for professionals |
|
See the evidence: eyes with a central corneal thickness of 555 µ or less have a 3 times increase in risk of progressing compared to eye with a thickness of 588 or more. Treatment in low risk cases can be safely delayed (Arch 2010). POAG can be predicted. |
Leaflet download |
| A Microsoft Publisher document, |
 |
| The address of this site ('org' changing to 'nhs') is changing from http://www.goodhope.org.uk/departments/eyedept/ to http://www.goodhope.nhs.uk/departments/eyedept/ |
|