Low Tension/Normal Pressure Glaucoma David Kinshuck |
|
|
What is glaucoma? |
|
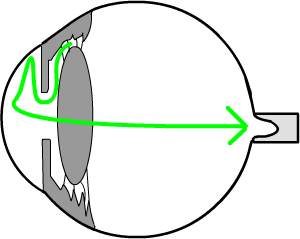
Glaucoma is a condition in which the nerve at the back of the eye is damaged. If severe, it can cause blindness, but most people do keep good sight indefinitely. It is explained in more detail on the Glaucoma page, which should be read in addition to this page. In ordinary glaucoma the nerve is damaged by an unusually high pressure in the eye. The high pressure stops the blood entering the tiny blood vessels in the part of the optic nerve that enters the eye.
|
In
ordinary glaucoma the nerve is damaged by pressure from a build
up of pressure inside the eye |
Low tension glaucoma |
|
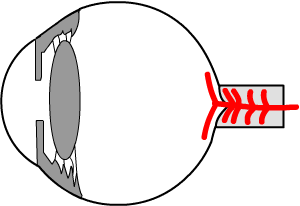
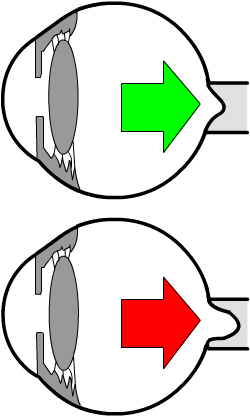
In this type of glaucoma we believe not enough blood reaches the
tiny arteries in the optic nerve. In low tension glaucoma it is thought the primary problem is too
low a pressure in the blood supply to the nerve. This is rather like
having a low water pressure in a house... not enough water comes
out of the tap. Treatment is drops in most patients. The drops lower the pressure in the eye so more blood can flow in. Occasionally an operation is needed as below. |
In low tension glaucoma not enough blood reaches the optic nerve (the tiny blood vessels supplying the optic nerve are shown in red). |
|
How does the treatment work? |
|
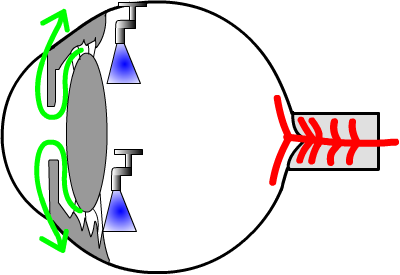
Normally, fluid (a little like water, called ‘aqueous humour’) is made in the middle chamber of the eye. It then flows through the pupil to the front chamber, and then out of the eye through small drainage channels. These channels are like a 'sieve' in the kitchen used to drain rice.
|
Aqueous fluid (green) is made in the
middle chamber of the eye (shown by the 'taps'), and drains out at
the side of the front chamber. |
Eye drops |
|
Eye drops containing drugs can ‘switch the tap’ off that makes the fluid (top half of eye opposite). Less fluid in the eye leads to a lower less pressure (like a tyre that is not pumped up as much). This allows more blood to enter the eye, and more blood flowing to supply the optic nerve. Other drops open up the drain that lets the fluid out (bottom half of eye opposite) |
 Less fluid is made (top half), or more fluid drains out of the eye. Both make the eye is softer and this lets more blood flow in to supply the nerve. enlarge |
|
An Operation |
|
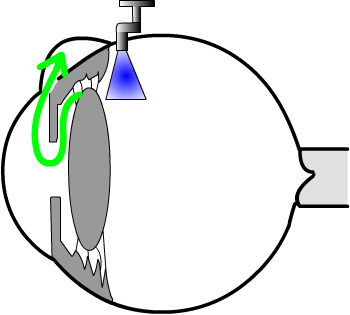
Occasionally an operation may be necessary. As part of the operation a small hole is made to let more fluid out of the eye. Your ophthalmic surgeon will discuss the pros and cons of the operation if it is necessary. |
A small hole is made at the top of
the eye, under the eyelid, to let the fluid drain out of the eye.
As a result, the eye becomes softer, and more blood can flow in. |
How is your sight affected? |
Usually the sight is not greatly affected in this condition. In younger patients (30-60y), the sight may get worse over many years. This can cause variable sight that changes during the day. Alternatively, the sight may be patchy, with clear areas and fuzzy areas. The damage can be similar to that of ordinary chronic glaucoma, as opposite. |
|
|||
Visual fields |
|
The sight is tested in the clinic for this type of patchy vision, by a visual field test. See a result. In this test, you have to put your head in a type of 'gold-fish bowl'. Lights are flashed on, and you have to press a button when you see the lights. The computer in the machine compares your result to that of a 'normal' person of your age, and prints out a serious of dots and black areas. The black areas are the area of damaged sight. |
Can you become blind? |
|
Only if you were very unlucky will your sight become very poor. Hardly
anyone becomes blind in that they cannot see anything at all, and only
occasionally will your sight become very bad.
If an ophthalmic surgeon recommends the drops, you should use them (unless you get side effects). Often the drops can make all the difference between keeping your sight and loosing it. (The same applies to an operation if your ophthalmic surgeon advises you strongly you should have one). Surprisingly, only two out of three patients recommended drops actually
use them regularly. If a doctor has advised to use the drops and
you choose not to, it is only fair to be honest and mention this
to your doctor. |
What tests do you need in the eye clinic? |
|
|
|
 |
|
A cupped, or damaged,
|
What can you do to help? |
|
See General health below. The main thing is to use drops if your doctor has advised you to. A few people have low blood pressure at night; ask you general practitioner if this is likely. There are no tablets and there is no magic cure though. Strangely, people with this type of glaucoma are more likely to have migraine or poor circulation in their hands (doctors call this 'Raynauds'). A low blood pressure is helpful (Kim 2010). Low tension glaucoma is related to general health vascular problems (Leung 2010). |
Your general health in glaucoma/intraocular hypertension |
|
Remember that your general health and lifestyle have a major impact on glaucoma and your sight. BJO 12
|
CNS changes |
There may be CNS changes in LTG. RCO 2011. |
Leaflet download |
|
this leaflet
This web page/leaflet is designed to accompany the Glaucoma page or Glaucoma leaflets available in an Eye Clinic; ask for one in your clinic if you have not seen one. |
 |
Notes for professionals |
Need careful
history
|
| The address of this site ('org' changing to 'nhs') is changing from http://www.goodhope.org.uk/departments/eyedept/ to http://www.goodhope.nhs.uk/departments/eyedept/ |
|