Retinal vein occlusion David Kinshuck |
|
|
What is a retinal vein? |
| The retinal veins are the small ‘pipes’ in the retina that drain blood out of the retina, back to the heart. |
 |
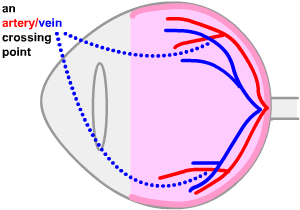
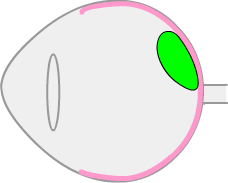
the veins of the retina may block: this is a side 'cut through' diagram of an eye |
| The retina is the thin film that lines the back of the eye, similar to the film of a camera. It is the part of the eye that makes us see. Light (things that you see) enters in through the front of the eye and falls on the retina. The retina turns the light into electrical signals that are sent to the brain, allowing you to see. The veins drain the blood out of the eye, whilst the retinal arteries are the small pipes that deliver the blood (from the heart) to the retina, shown in red in these diagrams. These arteries deliver the blood to the whole of the retina. |
What is a retinal vein occlusion? |
A retinal vein occlusion is a blockage of one of these veins. The vein blocks when blood in it stops flowing; then the vein cannot drain the blood out of the retina. When the vein blocks some blood leaks out. In addition, clear fluid leaks out causing ‘water-logging’ the retina. This naturally damages the sight. |
Where does the vein block? |
| It is that blood flowing through the vein may be blocked by something pressing on the vein. For example, any condition, such as high blood pressure for many years, that makes the small arteries ‘hard’, may cause the artery to press on the vein and block it. In a branch retinal vein blockage, the blockage is along the course of a retinal vein: |
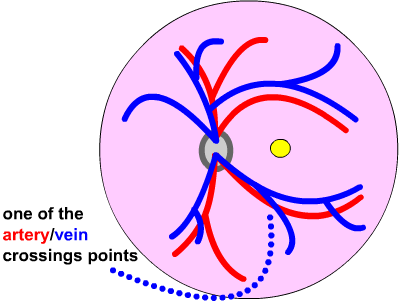
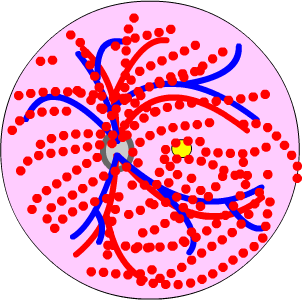
| A view of the retina from the front: what the doctor sees looking into your eye. The blue dotted line
points to an artery—vein crossing point, where the vein may be
blocked in 'branch retinal vein occlusion'.
|
 |
 |
enlarge |
In a central retinal vein occlusion, the blockage is at the optic nerve: |
|
 |
 |
| When is your sight affected? |
| The
centre of the retina is responsible for your sharp vision, such as seeing
people’s faces or watching television.
If this central part of the retina (a tiny yellow spot in these diagrams) becomes ‘waterlogged’ by leakage from the blocked vein, your sight will be reduced. After approximately 3 months, if the waterlogging remains, laser treatment may help to seal any leaks.
|
 |
Factors that contribute to retinal vein occlusion |
| High blood pressure | Controlling
the blood pressure helps to prevent the arteries getting ‘harder’,
and can prevent a blocked vein in the other eye. Some experts now believe
a blood pressure below 140/80 will not only help prevent
a second occlusion, but help reduce any retinal leakage from the one present
already. For information about blood pressure, visit |
|
| Too
much fat in the blood
|
A
healthy diet helps. The Department of Health (& World Health Organisation)
recommends people can help themselves by having
a balanced diet including:
Some experts recommend that many patients should use 'statin' tablets to lower their cholesterol, as this will also prevent heart and other diseases. (However, fibrates are preferable if the fasting triglyceride level is high.) Obesity quadruples the risk of a retinal vein occlusion, see. |
|
| Smoking | This
hardens all the arteries.
The more you smoke,
the more damage is done. Try to stop: ask your GP or nurse if you need help.
See
Smoking also contributes to cataracts, causing 25% of cataracts in the UK overall, and also 30% of macular degeneration. Smoking triples the risk of a retinal artery occlusion and carotid artery narrowing (and carotid artery narrowing is much more common in retinal vein occlusion patients, see) |
|
| Glaucoma, diabetes, and other conditions | Other conditions may also cause a blockage of a retinal vein (retinal vein occlusion, RVO), and extra treatment may be needed. Your doctor will check that you do not have one of these conditions. Sometimes the cause is not found. Patients with
glaucoma who develop an RVO
need to have a lower eye pressure. Patients with intraocular
hypertension need to be treated as though they have
early glaucoma, and need
a low pressure. High fibrinogen levels in the blood contribute to retinal vein occlusions, and these may be increased by stress or unhappiness, see If you are young or have had other venous occlusions, a check for other conditions may be needed. These include antiphospholipid antibody syndrome, factor V Leiden, or less commonly factor 5 or S abnormalities. For medical details see. Younger patients may need systemic steroids. If an RVO occurs in a patient with diabetic retinopathy, the outcome will be much worse...much more leakage, and new vessel development is much more likely. Sleep apnoea increase the risk. Patients with sleep apnoea need treatment and need to lose weight Archives 2010 |
|
Types of retinal vein occlusion |
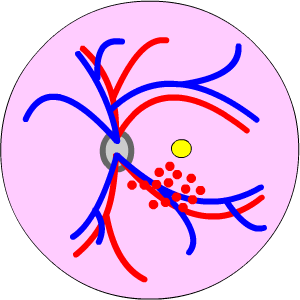
| A small ‘branch’ retinal
vein occlusion
If the central area of retina, the macula (shown in yellow) is not affected, the vision may be completely normal. The red marks show the 'haemorrhages' in the retina.
|
 |
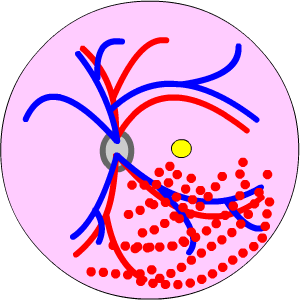
| A more
severe ‘branch’ retinal vein occlusion
Inevitably the central part of the retina is affected, reducing your sight, and laser is often needed. Laser treatment may be needed to reduce waterlogging, stabilising the sight. Hemispherical RVO review Retina 11 See photo (from mrcophth.com) and photo and larger and RVO case with large photos |
 |
| A central
retinal vein occlusion
Unfortunately, your sight is usually affected in this type of blockage. (Although a very mild blockage may not affect your sight.) Laser treatment does not improve the sight, but it may be necessary to prevent complications: tiny blood vessels can grow where they should not, leading to bleeding later. For medical details see. If the blockage is severe, a lot of laser is needed to prevent severe glaucoma (animation here). See photo (eyeatlas.com) |
 |
|
Retinal leakage |
|
some patients need treatment
to reduce waterlogging of the retina
|
 |
A retinal artery macroaneurysm |
This occurs when one of the tiny retinal arterioles at the back of
the eye block. A widened segment appears at the site of the blockage,
and this may start to leak. Subthreshold laser may help BJO 2011 |
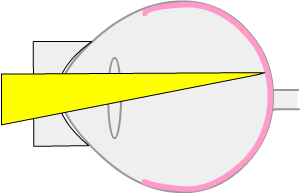
What is laser? |
| ‘Laser’ is a very
bright, but very narrow, beam of light. You need to sit in a machine
like the one used to examine your eye, and the light is shone in through
a small contact lens. If your condition is mild, the laser treatment does not usually hurt. (see Laser 2005) 2011 laser leaflet LASER is simply a highly focused and powerful light, where the light rays are all of the same type. For this reason it can be pointed at one spot very accurately. |
Laser light (yellow) is shone into the eye through a small contact lens, and makes small burns on the retina. |
Risk of rubeotic glaucoma / posterior segment neovascularisation/vitreous haemorrhage |
Risk of rubeotic glaucoma (Score 11)
Risk of posterior segment neovascularisation/vitreous haemorrhage (new vessel growth /blleding)
Risks are considerably reduced with laser. |
New treatments, including Avastin |
|
There are new treatments being developed. Although these treatments help in the short term, they may not help that much after a 2 year period or in the long term. Avastin research. Steroid injections
Anti-growth factor injections (Lucentis & Avastin)
|
What can you do? |
|
How to cope with poor vision in one eye |
| Ask your eye clinic doctor and optometrist, and see Coping with poor vision and Coping with poor vision in one eye. |
Leaflet download |
|
If you are a health professional and want to have a leaflet to give to patients, instead of this web page, see 200k Adobe PDF Alternatively, this is a Microsoft Publisher document click here, and you are welcome to download it and print copies. You are welcome to make changes for your patients (you can edit the leaflet in Microsoft Publisher). You will need M Publisher 2000 to open and print the document. M
Publisher is bundled as part of Microsoft Office. The only condition
is that you let me know if there are any errors. |
 |
| The address of this site ('org' changing to 'nhs') is changing from http://www.goodhope.org.uk/departments/eyedept/ to http://www.goodhope.nhs.uk/departments/eyedept/ |
|

{kind=link}
{kind=link}