New drug treatment for Neovascular ARMD: some notes David Kinshuck 2008 |
|
|
Lucentis, Avastin |
|||
These anti-VEGF drugs which are given as injections into the vitreous cavity of the eye see. They are very effective treating most types of wet ARMD. They are anti-growth factor drugs, and work by preventing the growth factor VEGF from working. VEGF stimulates the growth of the 'new blood vessels involved in neovascular ARMD, so when its effect is blocked the vessels close and the leakage stops. The VEGF is released from damaged retina. Although these drugs are effective, 'dry macula' changes still progress after treatment and sight can slowly deteriorate over years. Delays in use can cause visual problems. The benefits of Lucentis (Ranibizumab) are described in minimally classic/occult ARMD, and in classic. Monthly versus PRN |
|
||
Avastin Many ophthalmologists believe that Avastin (Moorfields) is just as effective as Lucentis, but it has to be given 'off label' in the UK; both are now approved in the US, but only Lucentis is licensed and funded for use in the UK. Avastin is much cheaper than Lucentis, and is made by the same company. All the research has been carried out with Lucentis, not Avastin. It is likely that this is because the company has a conflict of interests, and there is much less profit to be made from Avastin. Avastin is effective BMJ 2010 editorial 2010. Less frequent Avastin (every 12 weeks) is not as effective as frequent use Retina 2011. It is now official, Avastin is just as good as Lucentis, NEJM 2011 editorial. Another comparison Biswas 2011. In the US, Avastin is used twice as often as Lucentis AJO 2011, and is equally effective (College of Ophthalm statement 2011). |
|
||
Drugs combined with PDT etc |
|
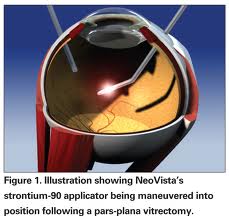
Brachy/radiotherapy |
|
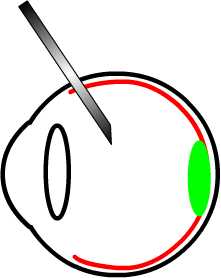
A surgical probe is inserted with a radioactive tip, and help in postion so the xrays treat the macular area. A vitrectomy operation is needed first. |
maculardegenerationdisease.com |
Current protocols (including NICE guidelines 2008) |
|
|
|
Anchor study |
Anchor is the main Lucentis and classic CNV study. |
|
Marina study |
Marina is the main Lucentis and occult CNV study. Aisenbrey's study. |
IVT: intravitreal triamcinolone |
| IVT is a steroid and can help reduce the size of CNV membranes. The procedure and risks are discussed here. With ARMD or CNV it is usually given in addition to PDT. and here . Concerning macular oedema in diabetes, Triamcinolone may reduce macular oedema more effectively. |
Lucentis & Avastin intravitreal injections |
The procedure is discussed here. (Triamcinolone has extra risks and is discussed here.) Avastin, infection..preventing These drugs are given as an injection into the vitreous cavity of your eye. They are given in a clean room or an operating theatre. The injection procedure itself takes seconds and is usually feels like a tiny prick. You can go home later that day...this is a 'day case' procedure'. |
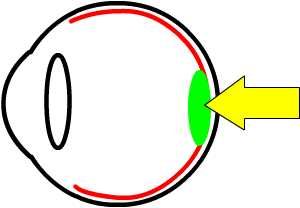
Macular degeneration shown in green by the arrow. Macular degeneration affects the centre of the retina which is responsible for sharp vision. The front of the eye is on the left, and the retina is shown in red. |
|
The eye is cleaned. Anaesthetic drops are instilled, and a few minutes later the nearly painless injection is given. The eye pressure may go up for a few hours, and extra treatment may be needed. You may see the drug floating around your eye for the next few weeks. |
|
After the injection |
After the injection you usually notice black swirls in the vision, which start to disperse gradually, but are a nuisance for a few weeks. By one month the drug should be working.
|
Risks etc |
Hours |
The injection will put the eye pressure up for a few hours. It is therefore riskier is you have glaucoma, but this is generally not a major problem. There should not be much pain. |
Days |
About 1/1000 people will develop a serious eye infection. The day after the injection your eye should be comfortable, there should
be very little pain. If your eye starts to get red, with misty vision
(there
may be no pain), perhaps 2-5 days after the injection, you should
suspect an infection and attend your eye department urgently. In Birmingham
this is the Birmingham
and Midland Eye Centre Casualty at the |
Risks summarised |
See this summary Rarely cataracts or retinal detachments may occur. Macular haemorrhages may develop (BJO 2008) . A rip may develop. Eye 2011. |
Anticoagulants ...extra precautions |
See ..You should remind your ophthalmic team you use anticoagulants and ask for specific advice. Treatment is safe continuing the anticoagulents (Retina 2010). Epidemiology 2010 |
Predictors of response |
"Thick Subretinal fluid and macular oedema on OCT may be characteristic of non-responders and may be helpful for tailoring treatment for neovascular AMD". See |
| The address of this site ('org' changing to 'nhs') is changing from http://www.goodhope.org.uk/departments/eyedept/ to http://www.goodhope.nhs.uk/departments/eyedept/ |
|